


In a milestone that signals a paradigm shift for the future of healthcare, a team of researchers and surgeons at the University of California San Diego (UC San Diego) has successfully conducted the world’s first teleoperated surgeries using humanoid robots. This proof-of-concept preclinical trial involved the successful removal of gallbladders—a procedure known as a cholecystectomy—in large, non-primate mammals. The achievement, detailed in a recent study published in the prestigious journal Nature, marks the first time a general-purpose humanoid form factor has been utilized to perform complex internal medical procedures, suggesting a future where versatile robotic assistants could replace or augment the massive, specialized machines currently dominating modern operating rooms.
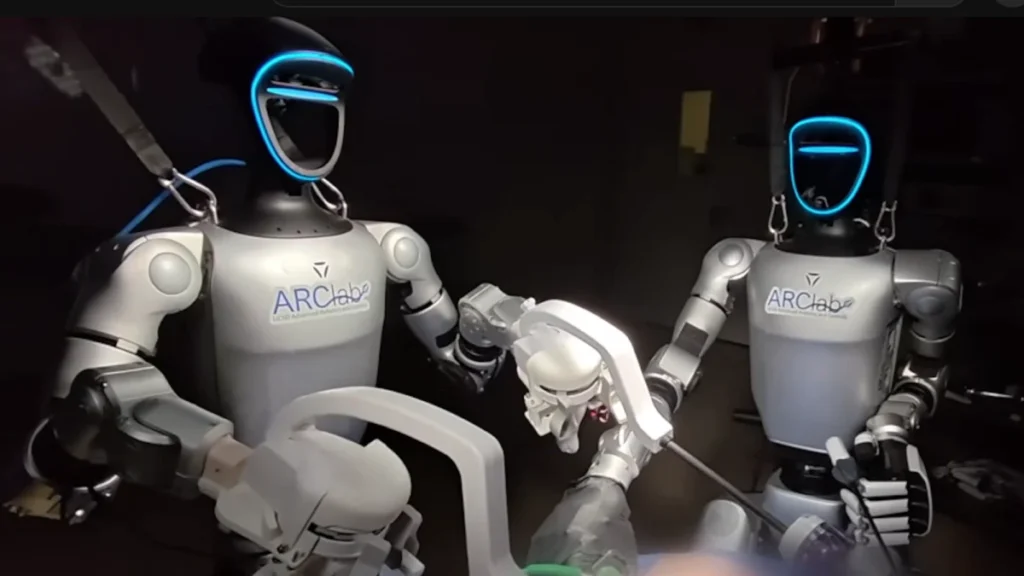
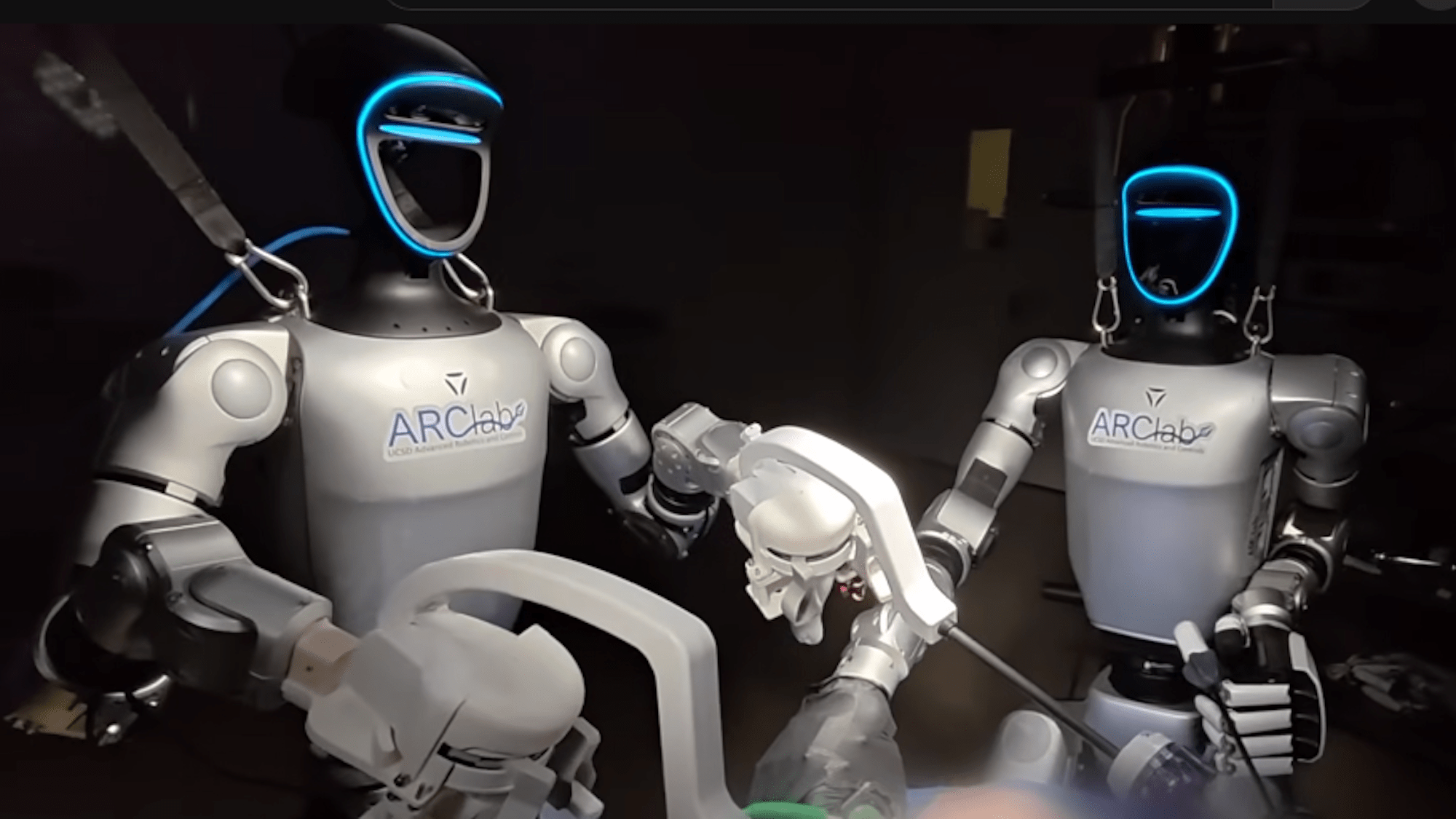
The trial was structured into two distinct phases to test the versatility of the robotic system. In the first procedure, a single humanoid robot worked in tandem with a human surgical assistant to complete the gallbladder removal. In the second, a pair of humanoid robots operated entirely under remote control to perform the same surgery. These "Surgie" bots, as they have been nicknamed by the development team, represent a departure from the "mainframe" era of robotic surgery toward a more mobile, adaptable, and cost-effective era of medical intervention.
The Evolution of Robotic Surgery: From Mainframes to Humanoids
To understand the significance of this breakthrough, it is necessary to examine the current landscape of robotic-assisted surgery. Since the early 2000s, systems like the Da Vinci surgical robot have become the gold standard in hospitals worldwide. These systems allow for minimally invasive procedures with high precision, but they come with significant logistical and financial burdens. Current industry-standard robots are massive, often weighing upwards of 1,800 pounds. They are fixed installations that require specialized, retrofitted operating rooms with reinforced flooring and dedicated power systems. Furthermore, these machines are typically "single-purpose" in their design; they are built specifically for surgery and cannot perform other tasks within a hospital environment.
In contrast, the Surgie robots developed at UC San Diego are designed for flexibility. Standing approximately five feet tall and weighing a mere 60 pounds, these humanoid units are lightweight and mobile. Their bipedal design and human-like limb proportions allow them to fit into existing operating room workflows without requiring the structural overhaul of the facility. While traditional surgical robots use a "spider-like" array of multiple arms emerging from a central pillar, the humanoid form factor utilizes two arms and a head-mounted camera system, mimicking the spatial presence of a human surgeon.
Michael Yip, an engineer at UC San Diego and a lead researcher on the project, emphasized the democratization of healthcare as a primary driver for this technology. "Remotely operated and autonomous humanoid robots have real potential for amplifying access to critical surgeries to which patients would otherwise not have access," Yip stated. He noted that the goal is to address the healthcare crisis not only within the United States but also in global regions where specialized surgical staff and expensive equipment are non-existent.
Technical Specifications and the Trial Chronology
The development of the Surgie platform required overcoming significant engineering hurdles, most notably the "tool-gap" between general-purpose humanoid hands and specialized surgical instruments. To bridge this, the UC San Diego team designed custom adapters that allowed the robots to grip and manipulate standard laparoscopic tools. These adapters enabled the robots to utilize the same scalpels, graspers, and cauterization tools that human surgeons use, rather than requiring the proprietary, high-cost instruments often mandated by traditional robotic systems.
The chronology of the trial began with the setup of a low-latency teleoperation station. Using a combination of motion-tracking suits and haptic feedback controllers, human surgeons were able to "pilot" the humanoid robots from a remote location. During the procedures:
- Preparation: The robots were positioned at the operating table, mirroring the stance of a human surgeon.
- Incision and Access: Under remote guidance, the robots successfully navigated the entry points into the abdominal cavity of the mammalian subjects.
- Dissection: The robots demonstrated the fine motor skills necessary to separate the gallbladder from the liver bed, a task requiring steady hands to avoid damaging surrounding vascular structures.
- Extraction: The organs were successfully removed, and the robots assisted in the closing of the surgical site.
Despite the success, the trial highlighted areas for improvement. The researchers noted that the Surgie bots required recalibration multiple times throughout the procedures, which extended the duration of the surgeries. Additionally, there was a measurable latency—a delay between the surgeon’s movement and the robot’s response—that required the operators to move more deliberately than they would in a traditional setting.
Comparative Data and Performance Analysis
The performance of the humanoid robots was evaluated against both traditional manual surgery and existing robotic platforms. While the humanoid surgeries were significantly slower than modern standards, the researchers pointed to the historical trajectory of laparoscopic surgery as a point of comparison. When robotic-assisted laparoscopic surgery was first introduced, initial procedures could take upwards of six hours. Today, those same procedures are routine and are often completed in under 30 minutes.
The data from the UC San Diego trial suggests a similar learning curve:
- Weight Efficiency: At 60 lbs, the Surgie robot is roughly 3% the weight of a standard 1,800 lb surgical system.
- Cost Reduction: The manufacturing and maintenance costs of humanoid units are projected to be a "fraction" of the multi-million dollar price tags associated with current medical robots.
- Spatial Footprint: The humanoid form factor occupies only the same floor space as a standing human, allowing for more personnel and equipment to remain in the operating room.
Dr. Shanglei Liu, a surgeon at UC San Diego and co-author of the study, highlighted the versatility of the system. "It’s easy to deploy, anywhere from rural areas to the battlefield, and even to space," Liu said. The ability to transport a 60-pound robot in a standard shipping container or even a large suitcase opens possibilities for surgical intervention in environments where it was previously impossible.
Reactions from the Medical Community
The response from the surgical team involved in the trial was one of cautious optimism and surprise at the "natural" feel of the interface. Nikita Thareja, a surgeon at UC San Diego who participated in the teleoperation, remarked on the seamless integration of the robot into the medical environment. "We were surprised at how well Surgie meshed with our workspace and workflow," Thareja noted.
Observers in the medical technology field have pointed out that the success of this trial validates the "generalist" approach to robotics. For decades, the trend in medical technology has been toward hyper-specialization—creating one machine for heart surgery, another for orthopedics, and another for imaging. The humanoid approach suggests that a single, well-trained robotic platform could eventually perform all of these tasks, as well as non-surgical duties such as patient transport, room sterilization, and instrument preparation.

Broader Implications: Rural Health, Combat, and Autonomy
The implications of successful humanoid teleoperated surgery extend far beyond the walls of urban teaching hospitals. In the United States, rural hospitals are closing at an alarming rate, often due to the inability to attract and retain specialized surgeons. A fleet of humanoid robots could be stationed at these rural outposts, allowing a specialist in a major city to "log in" and perform emergency surgeries hundreds of miles away.
In military contexts, the "Golden Hour"—the period immediately following a traumatic injury where medical intervention is most likely to prevent death—could be better utilized. Humanoid robots deployed near the front lines could be operated by surgeons located safely at base hospitals, providing immediate life-saving care on the battlefield.
Looking further ahead, the UC San Diego team is already eyeing the next frontier: autonomy. While the current trial relied on teleoperation (human-in-the-loop control), the ultimate goal is to develop an autonomous surgical assistant. This would involve the robot using artificial intelligence to perform routine parts of a procedure—such as suturing or suctioning—independently, while the human surgeon focuses on the most critical aspects of the operation.
"One of our goals is to develop an autonomous surgical assistant," Michael Yip explained. "Many communities struggle with adequate staffing on the surgical team, which means patients are not being treated. Our goal is an operating theater of the future, where humanoid robots and humans work side by side as an integrated team."
Conclusion and Future Outlook
The successful gallbladder removals at UC San Diego serve as a "Sputnik moment" for robotic medicine. While the technology is still in its preclinical stages and requires refinement in latency reduction and mechanical reliability, the proof of concept is undeniable. The transition from massive, immobile machines to nimble, humanoid assistants promises to make surgery more accessible, more affordable, and more adaptable to the needs of a global population.
As the team continues to refine the Surgie platform, future trials are expected to involve more complex procedures and longer-distance teleoperation tests. The path toward widespread adoption will require regulatory approval and extensive human clinical trials, but for the first time, the vision of a humanoid-assisted operating room has moved from the realm of science fiction into the reality of modern medical science.